Skip to search and filter Image ‘One Big Beautiful Bill’ Would Batter Rural Hospital Finances, Researchers Say June 13, 2025 Read more Image Opioid Stewardship Programs in Rural Arizona April 29, 2025 Opioid Stewardship Programs (OSPs) are a suite of tools to address substance misuse. Dr. Bridget Murphy, Assistant Research Professor at the University of Arizona Mel and Enid Zuckerman College of Public Health, aims to advance OSPs in rural areas. Read more Reporting from the front lines of rural health — before it’s too late April 23, 2025 Profile of Kaiser Family Foundation Health News' Rural Health Desk. Editor and Publisher Magazine Image Medicaid funding at risk: How will Arizonans be affected? April 21, 2025 Experts say millions of low-income people in the U.S. stand to lose their health insurance under Congressional Republicans' proposed budget for next year, which would end most federal support for Medicaid and shift costs to the states, who simply can not absorb the shortfall. "I estimate that probably 520,000 Arizonans that are currently covered by Medicaid will lose coverage," said University of Arizona associate vice president Dr. Daniel Derksen, director of the Arizona Center for Rural Health. "That's substantial. You're not saving money when you throw people off of coverage. You're just shifting the cost." Dr. Derksen quoted in Daily Wildcat Image Health care needs in Border Communities April 17, 2025 Dr. Derksen cited in ProPublica article discussing impacts of health care professional shortages for small rural community hospitals. Continue Reading the article from ProPublica Image Dr Derksen quoted in article on migrant health care March 27, 2025 In a look at the cost of health care for migrants in Arizona, Dr. Derksen weighs in on the hidden cost of not providing care. Read more Pagination « First First page ‹ Previous Previous page … 3 4 5 6 7 8 9 10 11 … Next › Next page Last » Last page
Image ‘One Big Beautiful Bill’ Would Batter Rural Hospital Finances, Researchers Say June 13, 2025 Read more
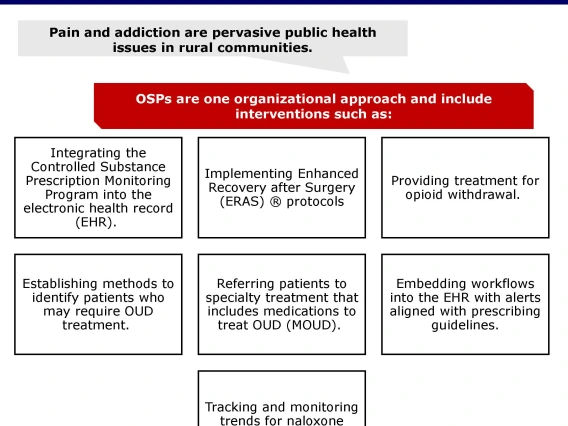
Image Opioid Stewardship Programs in Rural Arizona April 29, 2025 Opioid Stewardship Programs (OSPs) are a suite of tools to address substance misuse. Dr. Bridget Murphy, Assistant Research Professor at the University of Arizona Mel and Enid Zuckerman College of Public Health, aims to advance OSPs in rural areas. Read more
Reporting from the front lines of rural health — before it’s too late April 23, 2025 Profile of Kaiser Family Foundation Health News' Rural Health Desk. Editor and Publisher Magazine
Image Medicaid funding at risk: How will Arizonans be affected? April 21, 2025 Experts say millions of low-income people in the U.S. stand to lose their health insurance under Congressional Republicans' proposed budget for next year, which would end most federal support for Medicaid and shift costs to the states, who simply can not absorb the shortfall. "I estimate that probably 520,000 Arizonans that are currently covered by Medicaid will lose coverage," said University of Arizona associate vice president Dr. Daniel Derksen, director of the Arizona Center for Rural Health. "That's substantial. You're not saving money when you throw people off of coverage. You're just shifting the cost." Dr. Derksen quoted in Daily Wildcat
Image Health care needs in Border Communities April 17, 2025 Dr. Derksen cited in ProPublica article discussing impacts of health care professional shortages for small rural community hospitals. Continue Reading the article from ProPublica
Image Dr Derksen quoted in article on migrant health care March 27, 2025 In a look at the cost of health care for migrants in Arizona, Dr. Derksen weighs in on the hidden cost of not providing care. Read more