Skip to search and filter Image Thousands of Arizonans are at risk of losing health coverage if Trump cuts Medicaid Dec. 16, 2024 Dr Derksen quoted in Arizona Central article on Republican efforts to target health care. Changes to Medicaid are expected when President-elect Donald Trump takes office with a Republican-controlled Congress, and a potential target for spending cuts is the Medicaid expansion that was allowed through the federal Affordable Care Act, according to a Nov. 27 analysis by KFF, an independent health policy research and information organization. Read more Image 9 States Poised to End Coverage for Millions if Trump Cuts Medicaid Funding Dec. 9, 2024 Future of ACA in question, Arizona is one of nine states with trigger laws to end Medicaid expansion, Dr. Derksen is quoted. Read more Image Cancer can affect anyone. But Hispanics face disproportionately severe outcomes Nov. 20, 2024 AzCHOW, which serves primarily border communities and is located in Douglas, received over $500,000 from the Office of Minority Health this year to boost preventative efforts among underserved communities. The funding will go toward screening more adults for colorectal cancer and providing food vouchers. Read more Image Bipartisan Bill Introduced to Support Critical Access Hospitals Nov. 20, 2024 Bipartisan group of Senators introduced the Rural Hospital Flexibility Act, which would permanently reauthorize and modernize the Medicare Rural Hospital Flexibility Program. This program provides states with funding to support rural hospitals through training, technical support, and equipment for improving health care for patients, including emergency medical care. Read more Image Marc Verhougstraete starts prestigious fellowship in D.C. Nov. 13, 2024 Marc Verhougstraete, PhD, an associate professor of Environmental Health Sciences at the University of Arizona’s Mel and Enid Zuckerman College of Public Health, is participating in the American Association for the Advancement of Science’s Science & Technology Policy Fellowships this academic year. Read more Image CMS Announces New Policies to Reduce Maternal Mortality, Increase Access to Care, and Advance Health Equity Nov. 1, 2024 The Centers for Medicare & Medicaid Services (CMS) announced new baseline health and safety requirements for hospitals and Critical Access Hospitals (CAHs) providing obstetrical (OB) services to make pregnancy, childbirth, and postpartum care safer. Read more Pagination « First First page ‹ Previous Previous page … 5 6 7 8 9 10 11 12 13 … Next › Next page Last » Last page
Image Thousands of Arizonans are at risk of losing health coverage if Trump cuts Medicaid Dec. 16, 2024 Dr Derksen quoted in Arizona Central article on Republican efforts to target health care. Changes to Medicaid are expected when President-elect Donald Trump takes office with a Republican-controlled Congress, and a potential target for spending cuts is the Medicaid expansion that was allowed through the federal Affordable Care Act, according to a Nov. 27 analysis by KFF, an independent health policy research and information organization. Read more
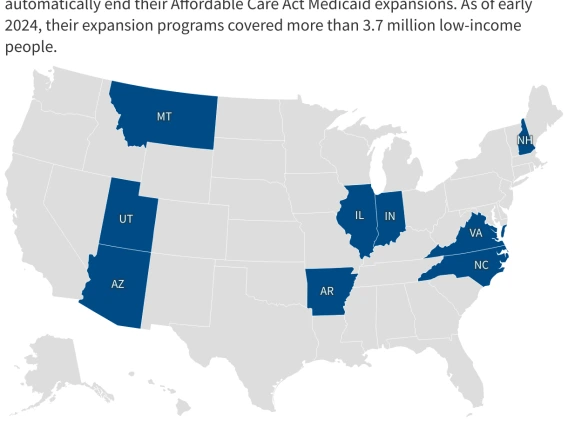
Image 9 States Poised to End Coverage for Millions if Trump Cuts Medicaid Funding Dec. 9, 2024 Future of ACA in question, Arizona is one of nine states with trigger laws to end Medicaid expansion, Dr. Derksen is quoted. Read more
Image Cancer can affect anyone. But Hispanics face disproportionately severe outcomes Nov. 20, 2024 AzCHOW, which serves primarily border communities and is located in Douglas, received over $500,000 from the Office of Minority Health this year to boost preventative efforts among underserved communities. The funding will go toward screening more adults for colorectal cancer and providing food vouchers. Read more
Image Bipartisan Bill Introduced to Support Critical Access Hospitals Nov. 20, 2024 Bipartisan group of Senators introduced the Rural Hospital Flexibility Act, which would permanently reauthorize and modernize the Medicare Rural Hospital Flexibility Program. This program provides states with funding to support rural hospitals through training, technical support, and equipment for improving health care for patients, including emergency medical care. Read more
Image Marc Verhougstraete starts prestigious fellowship in D.C. Nov. 13, 2024 Marc Verhougstraete, PhD, an associate professor of Environmental Health Sciences at the University of Arizona’s Mel and Enid Zuckerman College of Public Health, is participating in the American Association for the Advancement of Science’s Science & Technology Policy Fellowships this academic year. Read more
Image CMS Announces New Policies to Reduce Maternal Mortality, Increase Access to Care, and Advance Health Equity Nov. 1, 2024 The Centers for Medicare & Medicaid Services (CMS) announced new baseline health and safety requirements for hospitals and Critical Access Hospitals (CAHs) providing obstetrical (OB) services to make pregnancy, childbirth, and postpartum care safer. Read more